






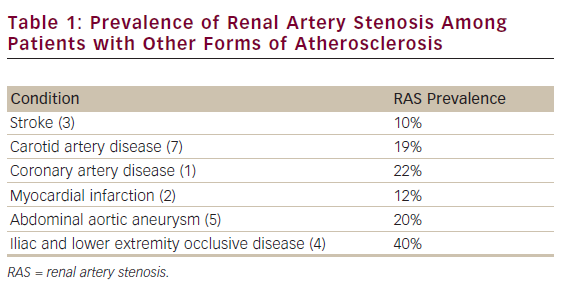
Renal artery stenosis (RAS) is a common manifestation of atherosclerotic disease. Although the exact prevalence rate for the population as a whole is unknown, RAS is seen in a significant proportion of patients who present with another manifestation of atherosclerosis (Table 1).1–7 Despite this high degree of prevalence, the management of RAS, specifically the role of revascularisation, remains controversial. Possible strategies for managing RAS span a spectrum of medical therapy-only at one end to a ‘find it and fix it’ revascularisation strategy at the other. In reality, the optimal strategy lies somewhere between these two extremes, with consideration of several patient-specific factors necessary to identify those who are candidates for revascularisation therapy.
Effects of Renal Artery Stenosis
RAS was identified as a potential cause of high blood pressure over 70 years ago, in the pioneering work of Goldbaltt.8 In addition to contributing to hypertension, RAS can also lead to decreased renal function – so-called ‘ischaemic nephropathy’, although the process is not just the result of a decreased oxygen supply, as the term ‘ischaemic’ would suggest. Other factors that might contribute to decreased renal function include the development of small vessel disease in conjunction with stenosis in the main renal artery. Additionally, embolic injury, triggered by main vessel RAS, might also contribute to renal dysfunction.
In addition to the direct effects of hypertension and decreased renal function, RAS can also lead to other adverse clinical events. Over 40 years ago, Wollenweber and Sheps reported increased cardiovascular morbidity and mortality among patients with RAS.9,10 Since then, numerous studies have consistently demonstrated an increased rate of adverse events among patients with RAS, compared with those without. Valentine and colleagues demonstrated an increased rate of coronary artery disease (CAD) among patients with RAS, compared with those without RAS (58% versus 39%).11 Conlon et al. reported a four-year survival rate among patients with RAS of 65%, compared with 86% for control subjects;12 Baboolal reported a similar survival rate of 55% for patients with bilateral RAS over a five-year follow-up period, as well as a 12% incidence of end-stage renal disease (ESRD).13 Among patients with both RAS and ESRD, the 5-year survival rate is less than 20%.14,15 Similarly high cardiovascular event rates among patients with RAS have been reported by both Johansson et al. and Kalra et al.16,17
Given these effects of RAS, management strategies are generally focused on improving blood pressure control and/or improving or stabilising renal function. Additionally, therapies should decrease the other adverse events associated with RAS. Such treatment strategies include optimal medical therapy and potentially revascularisation. The role of revascularisation for treating RAS remains controversial, with a divergence of results from retrospective analyses, case control and cohort studies when compared with the those of randomised clinical trials.
Revascularisation for Renal Artery Stenosis
Revascularisation for RAS includes both surgical and percutaneous techniques. Surgical techniques including endarterectomy, patch angioplasty, extra-anatomic bypass grafting and aortorenal bypass grafting are effective in restoring renal blood flow.18 Renal artery angioplasty was first reported during the late 1970s.19,20 This technique proved effective in improving renal artery blood flow; however, ostial RAS lesions were prone to high restenosis rates following angioplasty alone. The introduction of stents during the early 1990s resulted in improved acute outcomes, as well as decreased restenosis rates.21 As a result of high technical success rates and lower rates of complications compared with open surgical procedures, percutaneous revascularisation of RAS with stenting has emerged as the dominant revascularisation strategy.22,23
Evidence Supporting Revascularisation for Renal Artery Stenosis
There have been multiple publications that report benefit for percutaneous revascularisation in RAS. Most of these reports cite improvements in blood pressure or renal function as evidence of the benefit of revascularisation. In 1996, Iannone and colleagues reported that stenting improved systolic blood pressure and improved or stabilised renal function in a cohort of 63 patients.24 The report also identified renal insufficiency as a predictor of procedural complications. Similar results have been reported by other investigators in small groups of patients.25–27 In general, renal function improved or stabilised in approximately two-thirds of the patients treated with revascularisation. Blood pressure was reported as improved; however, this varied in terms of systolic versus diastolic.
In 2002, Dorros et al. reported follow-up data on over 1,000 patients enrolled in a multicentre registry.28 After four years, systolic and diastolic blood pressure decreased by 21 and 6mmHg, respectively. This decrease occurred in the setting of a concomitant decrease in the average number of antihypertensive medications from 2.4 to 2.0. Additionally, serum creatinine levels decreased from 1.7 to 1.0mg/dl. This study also suggested that survival was decreased among patients with elevated creatinine at baseline. The relationship between baseline renal function and follow-up blood pressure and renal function was not reported. A similar relationship between baseline renal insufficiency and an increased rate of adverse events following stenting for RAS was reported by Kennedy and colleagues.29 Importantly, this study suggested that, among patients with baseline renal insufficiency who had an improvement in creatinine following stenting, the rate of adverse events actually decreased.
In 2008, the results of the RESIST trial were published.30 In this trial, all patients underwent renal artery stenting, with randomisation to abciximab and the use of an embolic protection device in a 2x2 manner. When all patients were looked at, renal function decreased from baseline to one-month follow-up. This decrease in renal function was seen among control patients who underwent stenting without the use of abciximab or embolic protection, as well as among patients who only received either abciximab or embolic protection alone. However, among patients who received both abciximab and embolic protection, renal function at one month did not decrease. Notably, a subsequent analysis of data from the RESIST trial suggested that pretreatment with a thienopyridine before renal artery stenting might also be beneficial.31 Thus, the success of renal artery stenting might be dependent upon the selection of appropriate adjunctive therapies.
In 2010, the results of two multicentre registries of renal artery stenting were published. The results of the SOAR registry included a reduction in systolic blood pressure following stent placement that persisted to 36 months of follow up.32 Among all patients enrolled in the registry, serum creatinine levels increased slightly. Among patients with a baseline creatinine of 1.5mg/dl or greater, there was no significant change in creatinine at the 9–12 month follow-up evaluation; however, among patients followed for 24 or 36 months, serum creatinine increased.32
The ODORI registry reported a decrease in both systolic and diastolic blood pressure one year following renal artery stenting.33 Among all patients in the ODORI registry, renal function was unchanged at one-year follow-up; however, the subgroup analysis revealed some interesting trends. Patients were stratified by baseline estimated glomerular filtration rate (GFR). Patients with a GFR ≥60ml/min/1.7m2 had a significant decrease in GFR. Among patients with a baseline GFR ≥30<60ml/min/1.73m2, there was no significant change in GFR. In patients with a baseline GFR ≥15<30ml/min/1.73m2, there was a significant increase in GFR. Finally, in patients with a baseline GFR <15ml/min/1.73m2, there was also an increase in GFR; however, it was not statistically significant owing, in part, to the low number of patients in this subset. These registries suggest that stenting of RAS improves blood pressure and provides the greatest benefit upon renal function in patients who have impaired renal function at baseline.
Recently, Kalra and colleagues published a prospective cohorts trial of patients with RAS treated at centres in Germany and the UK.34 The UK cohort consisted of 347 patients treated with medical therapy and 89 patients who underwent revascularisation. Among the 347 patients treated conservatively, 45% had stage 3 chronic kidney disease (CKD) and 44% had stage 4 or 5 CKD. The German cohort consisted of 472 patients with 36% having stage 3 CKD and 14% having stage 4 or 5 CKD. All 472 patients in the German cohort underwent renal artery stenting. When all patients were analyzed, there was no significant difference between the two cohorts; however, patients with stage 4 or 5 CKD who underwent stenting were noted to have a significant improvement in GFR compared with those treated conservatively. Furthermore, among patients with stage 1 or 2 CKD, renal function deteriorated in both groups. A recent analysis of data from the RESIST trial also suggests that impaired renal function best predicts the patients most likely to have an improvement in renal function following stenting for RAS.35 Specifically, a GFR of 33ml/min/1.73m2 correlated with a 50% probability of improvement in renal function at one month. This probability increased as GFR decreased further and decreased as the GFR increased.
Evidence Supporting a Conservative Approach to Renal Artery Stenosis – The Randomised Trials
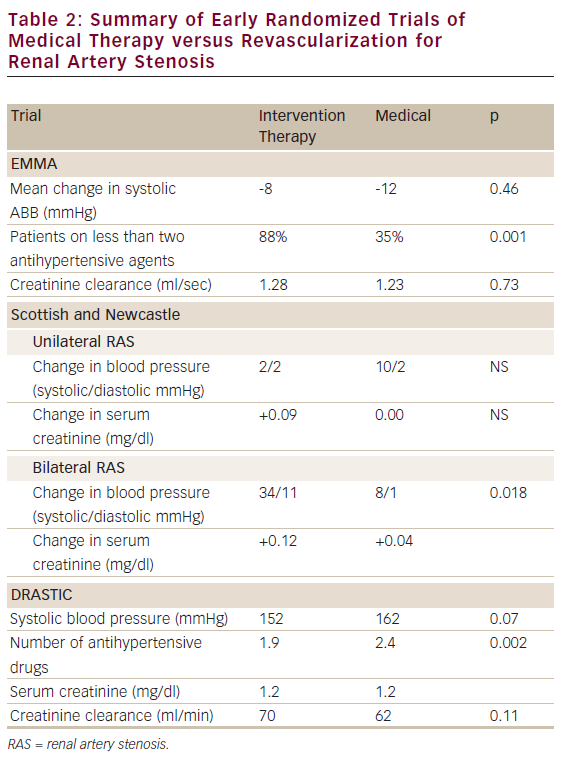
To date, the results of five randomised clinical trials of medical therapy versus revascularisation for RAS have been published. These trials can be grouped as early (published between 1998 and 2000) and late (published in 2009). The early trials include EMMA, the Scottish and Newcastle study, and DRASTIC.36–38 The results of these trials are summarised in Table 2. These trials were limited by low numbers of subjects, with a total of 210 patients combined. These studies were further limited by the fact that most of the patients underwent angioplasty without stenting.
In 2009, the results of the STAR trial were published.39 This trial compared renal artery stenting with medical therapy among patients with renal insufficiency, defined as a creatinine clearance of <80ml/min/m2. The primary endpoint was a worsening of renal function, defined as a 20% or greater decrease in GFR. There was no significant difference in the primary outcome between the medical therapy and stent arms of the trial. Although this trial was larger than the early trials and stenting was used, there were still several limitations. First, only 46 out of 64 patients randomised to stenting underwent the procedure. Second, there was a high rate of non-obstructive RAS, defined as <50% stenosis among enrolled patients. Finally, the degree of renal insufficiency in this trial was relatively mild. Many of the non-randomised studies already identified that the renal function benefits of stenting are seen in patients with at least moderate (stage 3 CKD) renal insufficiency. Thus, it is not surprising that, among patients with mild RAS and mild renal insufficiency, there was no benefit with regards to renal function following stenting.
The ASTRAL trial was also published in 2009.40 ASTRAL was a large study with 806 subjects with RAS randomised to revascularisation or medical therapy. The primary end-point for the trial was renal function with a mean follow-up period of 33.6 months. The slope of the reciprocal of the serum creatinine concentration was -0.13x10-3l/mmol/year in the medical therapy group compared with -0.07x10-3l/mmol/year in the revascularisation group. The p-value for this difference was 0.06. Additionally, there was no significant difference in secondary outcomes, including blood pressure control, renal events and cardiovascular events. As with the other randomised trials of revascularisation for RAS, ASTRAL had several limitations.
First, a large percentage of the enrolled patients had only moderate RAS and this was not verified by angiographic core lab analysis. Thus, the actual degree of RAS among enrolled patients was probably even less severe as physicians tend to overestimate percent stenosis. Furthermore, although renal function was the primary endpoint for this trial, a substantial number of patients were enrolled who had normal to mildly impaired baseline renal function. Thus, as with the STAR trial, it is not surprising that there was limited benefit seen with stenting.
Ongoing Randomised Trials
Currently, there are two ongoing randomised trials of medical therapy versus stenting for RAS. The CORAL trial completed enrollment in January 31, 2010, with final follow-up expected in March, 2014. The primary end-point for this trial will be a composite of cardiovascular or renal death, stroke, myocardial infarction (MI), hospitalisation for congestive heart failure (CHF), progressive renal insufficiency or the need for permanent renal replacement therapy.41 The RADAR trial is another prospective randomised trial of renal stenting compared with medical therapy for RAS.42 The primary end-point for RADAR is the change in GFR over 12 months. The results of these two trials will help further clarify the role of revascularisation for patients with RAS.
Perspective
To date, randomised trials have failed to show a benefit of revascularisation in RAS. Nevertheless, there is a large body of evidence from registry and cohort studies suggesting that revascularisation is beneficial for RAS. Although additional trials are ongoing, controversy remains. Based upon available data, what is a physician to do when faced with a patient with RAS? First, a ‘find it and fix it’ strategy based upon the belief that an open artery must be better is overly aggressive. By contrast, adopting a medical therapy-only strategy, based upon the randomised data, might not be appropriate. Each patient needs to be carefully evaluated, and all aspects of their condition considered, before deciding upon a given course of action.
When encountering RAS, a physician should first determine what the treatment goals are. If hypertension is an issue, it is first important to optimise medical therapy to reduce blood pressure. If blood pressure remains uncontrolled despite three or more agents from different pharmaceutical classes, all at high doses, then stenting for RAS can be considered; however, although there might be some blood pressure benefit with stenting, it is unlikely to cure hypertension. If there are concerns about renal function, stenting should probably not be considered until a patient has at least stage 3 CKD. Although patients with more advanced CKD might be at increased risk for adverse events, they also seem to derive the greatest renal benefit from stenting. Thus, this group of patients truly represents a ‘high risk–high reward’ group.
Physicians who keep up to date regarding the management of RAS and who thoughtfully consider the best course of action for a given patient are most likely to achieve good outcomes. Until the time, if ever, that a consensus arises from the data, no single study will be able to replace the careful consideration of a thoughtful physician.