






Transfemoral access (TFA) has been widely used in interventional neuroradiology and is the most frequently used vascular approach for catheterisation of the supraaortic and intracranial vessels. However, TFA can lead to potentially life-threatening complications, which has sparked interest in transradial access (TRA) as a safer access option. In a review of 19,826 consecutive patients undergoing diagnostic cerebral angiography using TFA, access-site haematoma was the most common complication overall (4.2%).1
Percutaneous radial access was described by Campeau in 1989 for coronary angiography in 100 patients.2 Since then, a growing body of evidence suggests that TRA is safer for patients and more cost-effective compared with TFA. Radial access reduces mortality and major adverse cardiovascular events and improves safety, with reductions in major bleeding and vascular complications across the whole spectrum of patients with coronary artery disease.3 The 2018 European Society of Cardiology/European Association for Cardio-Thoracic Surgery guidelines on myocardial revascularisation state that radial access is preferred for any percutaneous coronary intervention irrespective of clinical presentation, unless there are overriding procedural considerations.4
Matsumoto and colleagues described TRA for neurointervention procedures in 2000 and there are large series showing the safety and feasibility of transradial cerebral angiography.5–9 Furthermore, complex interventions for both ischaemic and haemorrhagic disease of the posterior and anterior circulation have been reported, highlighting the feasibility of this approach despite the use of femoral-designed devices.10–16 Adoption of TRA has been slow in the neuroendovascular field, although interest has increased in recent years.
In this review, we examine the advantages, limitations and technical details of neurovascular interventions using TRA. Specific technical details for neurointerventions in haemorrhagic and ischaemic disease are also described.
Advantages
The vast experience of using TRA in cardiology has yielded considerable knowledge about its safety, although some specific conditions regarding neurointerventions need to be considered. Because of its recognised safety, TRA might be the first option in patients with severe femoral or aorto-iliac disease, obese patients with deep femoral arteries or patients with high haemorrhagic risk. Anticoagulants do not need to be withdrawn when using TRA in patients receiving these medications. Even though it is not well established that TRA is necessarily safer in patients with atherosclerotic disease involving the aortic arch for neuroendovascular procedures, it is known that in the thoracic region calcifications are more often formed in the aortic arch and descending rather than ascending aorta.17,18 For some TFA-challenging anatomies such as a bovine or type III aortic arch type, TRA might be a better option. TRA also has the advantage of offering direct access to the vertebrobasilar system. Other TRA access advantages include better tolerability and short haemostasis times allowing for very short hospital stays – both in diagnostic angiographies and scheduled interventions. From a financial perspective, there are savings in access complication costs, closure devices and hospital stay.19
Limitations, Crossovers and Complications
Despite the feasibility and known advantages of TRA, there are access site and cerebrovascular-specific limitations to TRA. In the field of cardiology, recent registries have shown that risk of access failure and conversion to TFA has a low conversion index (1.5%), due to operator experience, improved techniques and material.20,21 This contrasts with older trials, in which the failure index was 7.3% compared to 2% for TFA.22
There are data showing that experience performing approximately 30–50 TRA cerebral angiograms is needed to become comfortable with TRA. During the learning curve, there is a reduction in crossover rate and fluoroscopy times, with better success in catheterising all intended supra-aortic arteries.23,24 In a recent systematic review of 1,342 procedures of TRA for neurointerventions, the crossover rate to TFA was 4.77%. Among the crossover group, 10.93% crossed over because of the failure to obtain radial artery (RA) access and because of the inability to catheterise the target vessel in 89.06%.25
The two most common complications associated with TRA are RA spasm and RA occlusion. RA spasm is noted in 15–30% of cases, but this can be reduced to 6–10% with intra-arterial administration of nitroglycerin and a calcium channel blocker.26,27 RA occlusions have been reported to occur at rates of 0.8–33% in different series, but this can be reduced significantly with precautions described in the following section.20,28 Furthermore, RA occlusion is clinically silent in the majority of cases, secondary to collateral circulation via the palmar arch. Apart from difficulty using the same RA for future access, the clinical implications of RA occlusion are very limited.29,30
Clinically relevant complications, such as hand ischaemia requiring amputation and compartment syndrome, have been reported, but are exceedingly rare.31 Minor complications, such as extended access site pain, haematoma and bruises, are other possibilities.32 There are some anatomic variations of the RA that operators should be aware of, such as high brachial artery bifurcation, radial or brachial artery loops, tortuosity of the RA and the presence of an accessory RA.
For cerebrovascular angiography specifically, some challenging anatomies may cause difficulty in catheterisation of the vessels. These include the left vertebral artery, a proximal right common carotid artery (CCA) with an acute angle or a loop in the left CCA. Another anatomic variant, subclavia lusoria (reported to be present in 0.1–0.8% of cases) may present some catheterisation difficulties from a right TRA.33
Technical Details
Pre-procedure
Traditionally, assessment of the collateral circulation to the hand via Allen’s test and the Barbeau test (objective Allen’s test using pulse oximetry and plethysmography) has been used prior to TRA. However, significant controversy exists regarding the need for pre-procedural collateral circulation testing.34
Of note, the Minimizing Adverse Haemorrhagic Events by TRansradial Access Site and Systemic Implementation of angioX (MATRIX) trial randomised more than 4,000 patients to TRA (regardless of the pre-procedure collateral testing result) and found no post-procedure symptomatic hand ischaemia.35
Size Matters
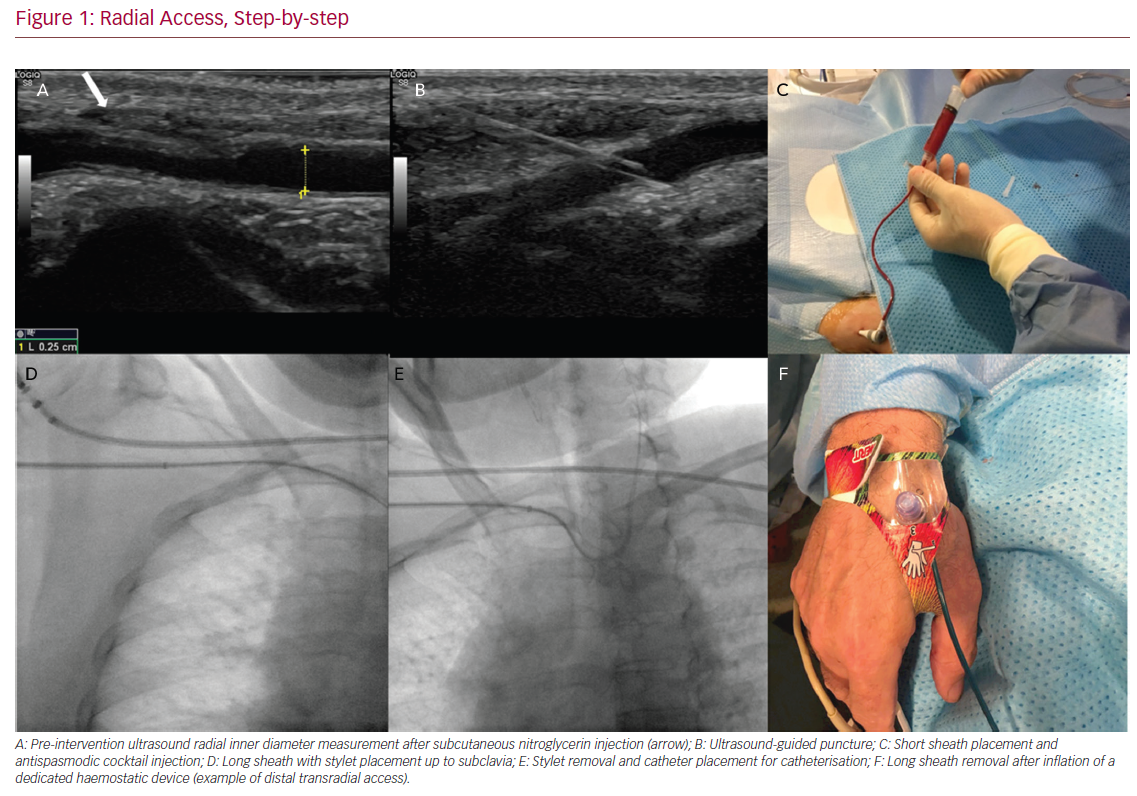
The RA – having a smaller calibre – has a series of limitations regarding the diameter of the materials used and, in some patients, this may preclude its use.36 In our experience, the use of ultrasound both for puncture and to measure the diameter of the artery serves to correctly select and rule out radial procedures in patients in whom the radial inner diameter is <1.5 mm (Figure 1). It is important to note that when measuring the diameter of the artery there are factors that can influence the results (check that the patient is not cold and is calm).
Several authors have analysed the diameter of the RA with ultrasound and correlated the risk of occlusion depending on the external diameter of the introducer used.21 They found no correlation of the radial diameter with BMI.22 A cannulation procedure can still be attempted with smaller radial diameters, but the chances of vasospasm and TFA conversion are higher, especially in young women.37 Administration of topical lidocaine and nitroglycerin or subcutaneously administered nitroglycerin prior to puncture has been shown prospectively to increase the diameter of the RA and facilitate TRA.34,38,39
In most patients, performing a diagnostic angiogram with a 5 Fr introducer will be possible. A cross-sectional inner RA diameter of approximately 1.5–2.0 mm is required for a 5 Fr sheath and diagnostic catheters. Some interventions can be done through a 6 Fr or 7 Fr thin-walled specific radial sheath, from which a 6 Fr (0.070 inner diameter [ID] system) or 7 Fr guiding catheter can be used. For a 6 Fr sheath, we recommend at least 1.9 mm of radial diameter. The Terumo slender 6 Fr and Prelude Ideal (Merit Medical) thin-walled specific radial sheaths have an outer diameter of 2.44 mm compared to other non-thin-walled radial sheaths (2.63−2.8 mm) and Terumo 6 Fr femoral sheaths (2.62 mm). Other interventions may require larger sheaths and intermediate catheters for support. In our institution, for cases in which large-bore sheaths (0.088 ID) are needed, this approach is used if the radial diameter is at least 2.3 mm.
Prevention of Spasm and Occlusion
While essentially clinically silent, prevention of RA occlusion is important, especially with regard to consideration of further procedures. RA occlusion rates have been shown to increase with increasing sheath diameter, especially when the outer diameter of the sheath exceeds the inner diameter of the RA. The use of sheathless TRA has been described as allowing for larger ID guide catheters to be placed without an attendant increase in outer diameter from sheath placement.40
Administration of unfractionated heparin at therapeutic levels (50 IU/kg or 5,000 IU) has been shown prospectively to lead to a sixfold reduction in RA occlusion rates, with higher rates of administration (100 IU/kg) further decreasing the incidence of RA occlusion.41,42 However, the best route for heparin administration remains unclear, with no difference between intravenous and intra-arterial bolus administration through a sheath with regard to RA occlusion rates.41–43
The administration of intra-arterial antispasmodic medications has been shown prospectively in multiple trials to reduce RA spasm although without a clear consensus on the most effective combination and dose.44–46 A meta-analysis of 22 randomised trials found the lowest rates of RA spasm following intra-arterial administration of nitroglycerin 200 µg and verapamil 5 mg.47 We recommend preparation and administration of a cocktail in a 20 ml syringe with 200 µg nitroglycerin, 5 mg of verapamil and 4,000 IU heparin. Once the sheath is in place, we aspirate blood to fill the 20 ml cocktail syringe and inject it gently to minimise discomfort. Recalcitrant RA spasm can be managed with further administration of antispasmodic medications.
Closure
The use of a patent haemostasis technique significantly improves RA patency rates. Patent haemostasis has been shown to reduce rates of RA occlusion by 75% compared with conventional pressure application, either manually or with a compressive haemostatic band.48 Prophylactic ulnar artery compression, added to patent haemostasis, is reported to result in RA occlusion rates <1%.49 Although use of patent haemostasis is paramount in preventing RA occlusion, there is no consensus on the optimal protocol for deflation of the radial haemostatic band.48 If RA occlusion is encountered immediately post-operatively, ulnar compression, as well as administration of low-molecular-weight heparin can promote recanalisation.50
Distal Transradial Access
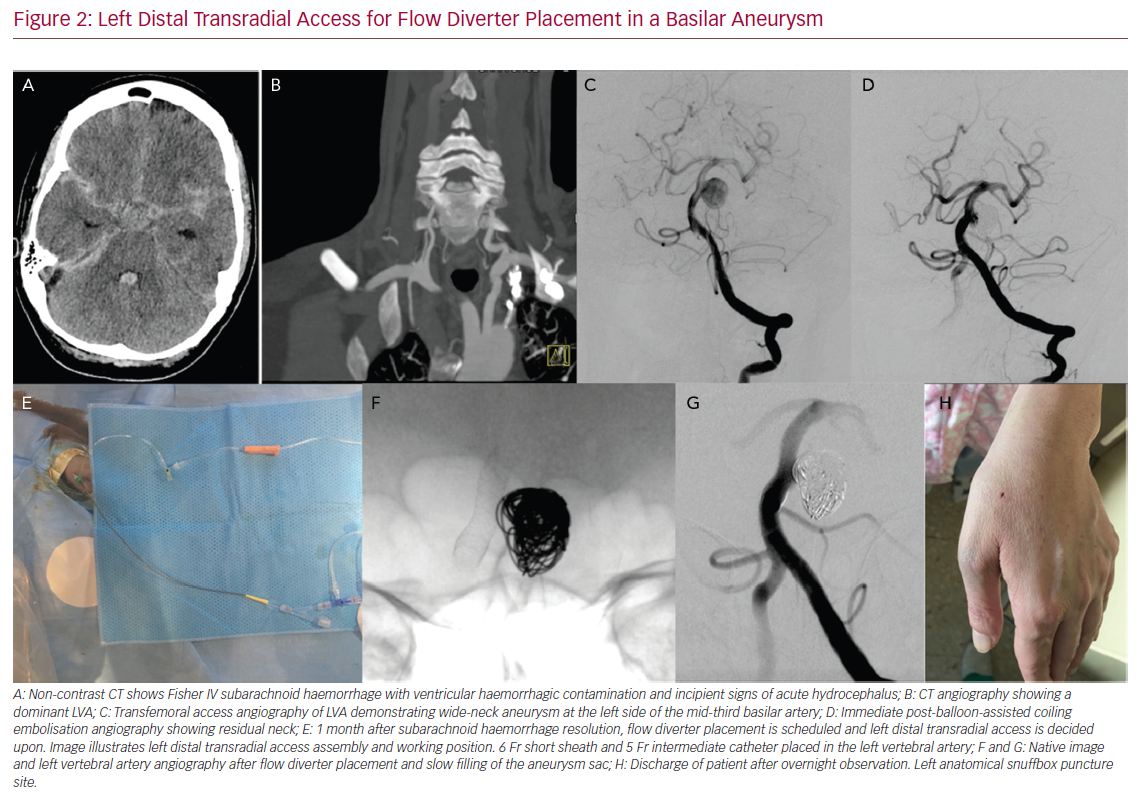
Recently, distal transradial access (dTRA) has received more attention in the attempt to improve some of the limitations of conventional radial access.51 Recent series have reported both cerebral angiography and neurointerventions successfully performed through dTRA.52,53 In puncturing the RA in the anatomic snuffbox, distal to the origin of superficial palmar branch, in the case of occlusion there is a theoretically lower risk of compromising the superficial palmar arch and less risk of hand ischaemia. In addition, the forearm can be kept in mid-prone position right next to the body, which reduces discomfort because the position is more ergonomic. In interventions in which left RA is needed, it is very difficult to use the left conventional radial approach as most neuro suites are designed (e.g., the position of controls and the screen) to work on the right side of the patient. In these cases, left distal radial access is particularly useful to perform left vertebral artery procedures via the left forearm. The left forearm is kept partially flexed over the patient’s abdomen with the hand close to the left groin and then taped in place (Figure 2).
The diameter of the distal RA, which can be smaller in the snuffbox compared with the conventional radial puncture site therefore predisposing to spasm, may result in higher conversion rates.54 We strictly recommend the use of ultrasound to measure, select, and puncture the distal RA at the snuffbox.
Another advantage of puncturing the dTRA is that patency rates are reported to be very high and this permits short haemostatic protocols.55 In addition, in the case of artery occlusion, this normally happens at the level of the snuffbox. Therefore, the RA can still be punctured in the forearm.
Haemorrhagic Disease
Because haemorrhagic disease can involve both acute ruptured disease or elective cases, we recommend first trying radial access in elective rather than acute cases. During this kind of intervention – in which larger diameter catheters and sheaths might be used – sedation and general anaesthesia also help to reduce the incidence of RA spasm by reducing both anxiety and sympathetic drive.56,57
Aneurysm Treatment
A 6 Fr short sheath can be used to introduce a 0.070 ID system after spasmolytics are administered. The 0.070 ID system can either be a Simmons-2 guiding catheter Envoy (Codman Neuro) or any other guiding catheter using a long Simmons-2 catheter or using a wire exchange. In the event that simple coiling is used, a 6 Fr catheter such as Envoy DA may allow the use of a 0.058 intermediate catheter if needed (e.g. a 5 Fr Navien [Medtronic] or 5 Fr Sofia [Microvention]). Most aneurysm embolisation techniques can be performed through
a 6 Fr guiding catheter, which allows two microcatheters in order to perform balloon-assisted coiling (BAC) and/or stent-assisted coiling (SAC). In more challenging cases where greater support is needed, larger sheaths and intermediate catheters may be required.
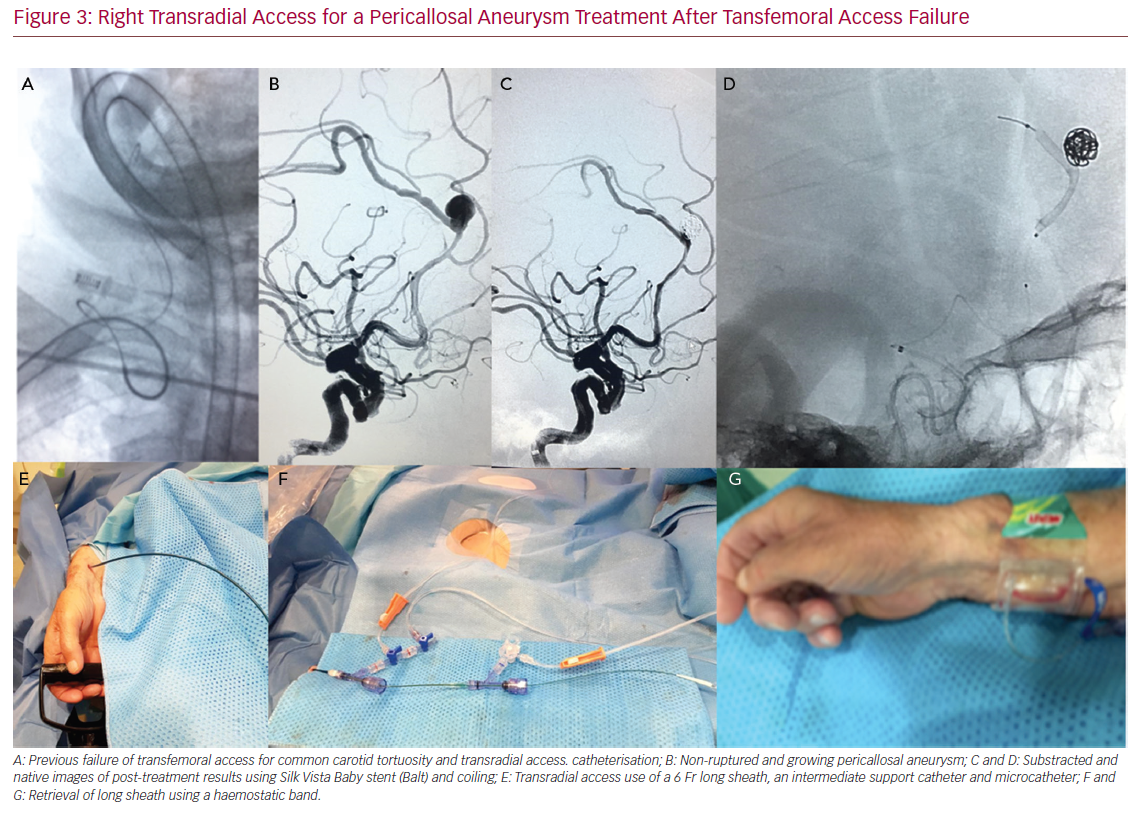
For treatments in which a large-bore sheath (0.088 ID) is needed, we would recommend that the RA size be at least 2.3 mm in cross-sectional diameter. To use them, we perform an exchange of the short sheath (after the injection of a spasmolystic) by placing a guidewire in the subclavia. The short sheath is removed, and a long sheath is then advanced into the RA over the wire. Similar to TFA, a small skin incision might be necessary prior to advancing the large-bore sheath. The stylet is then removed, and a Simmons-2 shaped catheter is navigated over a guidewire into the target internal carotid artery (ICA) and then the Simmons shape is reformed in the arch. Once the catheter is in the CCA, a guidewire is advanced into the ICA. The catheter can be advanced over the guidewire to the ICA, and then the long sheath is advanced over the Simmons catheter. Simmons catheters may not advance easily over the wire and tend to herniate in the arch. This problem can be solved with a stiffer 0.35 guidewire or by advancing the long sheath while the guidewire is in the ICA and the selected catheter is in the origin of the CCA. Our institutional experience is using catheters such as Shuttle (Cook Medical) and more recently Ballast (Balt). A large-bore 6 Fr long sheath allows using a 6 Fr intermediate catheter, which can provide enough support to deploy flow diverters14 and offer better support for BAC or SAC (Figure 3).
In some embolisation cases where a double access is needed to control both carotids, both vertebral arteries, a posterior and anterior circulation artery, or to do a transcirculation approach, TRA can be also useful.58 Access can be through both RAs or combining TRA and TFA. In cases with ruptured aneurysms, we tend to administer the radial cocktail without heparin and give systemic heparin once the first coil is detached and BAC is performed. The decision as to when to give heparin depends more on the need for neurovascular intervention and safety rather than prevention of RA occlusion. In our experience, the use of radial access for elective aneurysm embolisation also allows early patient discharge after overnight observation.
Treatment of Arteriovenous Malformation and Arteriovenous Fistula
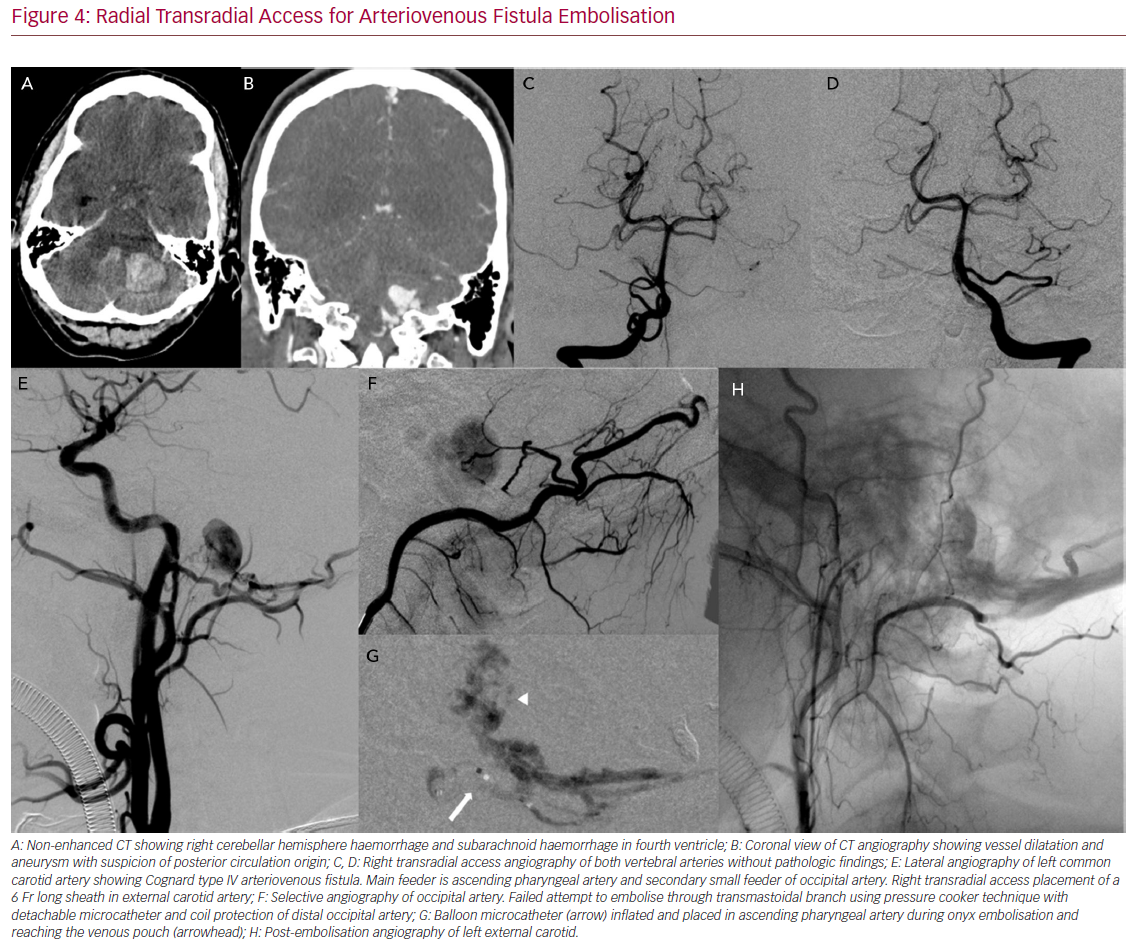
Complex interventions such as arteriovenous malformation (AVM) and arteriovenous fistula (AVF) embolisation can also be done through TRA (Figure 4). In cases of a multiple feeder AVF or AVM, double access may be required. While one access can be the treating one, in other vessels diagnostic catheters may help to ensure all the feeders are closed. TRA can be used as the main treating access, as a control catheter access or as a multiple access from both radial arteries (for the left radial a left dTRA is recommended).
Most embolisation techniques, such as single microcatheter, balloon assisted embolisation, pressure cooker technique with an Echelon-10 (Microvention), and detachable tip microcatheter can be applied through a 6 Fr guiding catheter and a 6 Fr radial sheath.59 When the pressure cooker technique with magic catheter is required, a 6 Fr long sheath or a 7 Fr guiding catheter through a 7 Fr radial sheath can be used.59
A specific potential drawback of TRA for this kind of intervention is the need to work with low blood pressure and not administer systemic heparin.
Ischaemic Disease
Stroke Thrombectomy
As is commonly recognised, stroke revascularisation has a crucial difference compared with other neurovascular procedures in that not wasting time is mandatory.
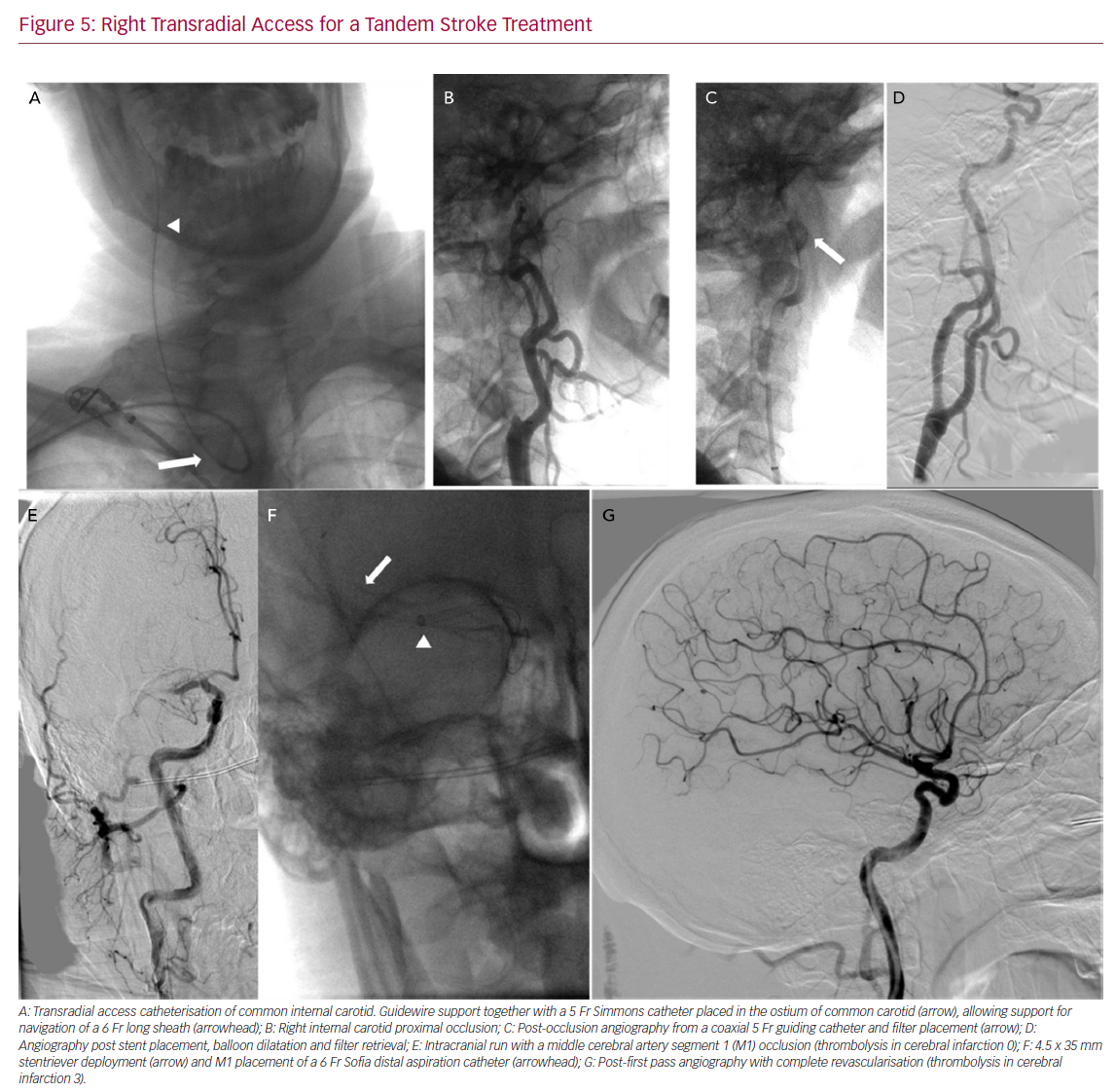
In our experience, we have performed TRA thrombectomies once both the operator and the rest of the team have gained enough experience performing diagnostic angiographies and other interventions. Even with experience, the first TRA cases were done after TFA failure. With experience, cases can be selected to do TRA as a first approach in vertebro-basilar stroke, bovine arch and type III aortic arch. One potential advantage of TRA over TFA is that the smaller radial and brachial diameter acts as a support to the system when dealing with vascular tortuosity. Some authors have compared TRA and TFA performance in stroke thrombectomy in different challenging aortic anatomies,60 demonstrating its feasibility (Figure 5).
Before proceeding with a TRA we first measure the RA inner diameter and rule the procedure out if the diameter is <2.3 mm in order to minimise the risk of RA spasm. The simplest means of performing the thrombectomy is with a stentriever while aspirating from a 6 Fr guiding catheter placed in the ICA through a 6 Fr specific radial sheath. Either a Simmons-2 shaped 6 Fr Envoy guiding catheter placed directly, or a 6 Fr guide catheter coaxially navigated into the target ICA over a 125 cm Simmons-2 shaped diagnostic catheter can be used. However, this technique means not using a distal aspiration catheter as a proximal occlusion balloon.10
For anterior circulation stroke, in the case of the Direct Aspiration First Pass Technique (ADAPT) or distal aspiration with retrievable stent assisted thrombectomy, a large 6 Fr sheath is required.
As previously described, a 6 Fr large sheath can placed in the ICA, having enough support through the arch and allowing aspiration catheters up to 0.71 inches, such as Penumbra ACE 6 (Penumbra) Sofia 6 Fr+, React 071 (Medtronic), or AXS Vecta 71 (Stryker). Having a 6 Fr long sheath in place also allows treatment of tandem stroke, and, if required, carotid stents can be place through it.
For operators who prefer using balloon occlusion aspiration, there are several options:
- When the radial diameter is small, a 7 Fr radial thin-walled sheath allows a Cello 6+ balloon guide catheter (Medtronic).
- Once a Simmons catheter is introduced into the 7 Fr sheath and used to navigate to the target ICA over an exchange guidewire, the catheter is removed and the Cello balloon guide catheter is advanced. One possible disadvantage of this technique is that as the balloon inner diameter is smaller there is a theoretically greater risk of catheter occlusion in cases with high thrombotic burden.
- When in the pre-procedural ultrasound radial diameter is at least 2.4 mm, an 8 Fr balloon guide catheter can be used.
We recommend doing this sheathlessly, without an 8 Fr short sheath. Both Cello 8 Fr (Medtronic) and Merci 8 Fr (Stryker) have stylets, and can be placed as previously described with long sheaths, by wire exchange from a previously placed short sheath. Once the balloon tip is placed in the subclavian artery, the stylet can be removed and replaced by a Simmons-2 shaped catheter. The Flowgate 2 balloon (Stryker) package has a 6 Fr catheter instead of a stylet, which might be used as well making a prior skin incision almost mandatory.
More data are needed regarding the safety of prophylactic heparin administration to prevent RA occlusion owing to the risk of haemorrhagic conversion after stroke. Most centres perform thrombectomy without systemic heparinisation, even though some heparin is infused through the saline perfusion of the catheters.
In our experience, in those cases with bridging therapy and previous recombinant tissue plasminogen activator, we do not administer heparin to prevent RA occlusion. In other cases, once the procedure is finished without complications, we administer lower heparin doses (2,000 IU) just before retrieving the sheath from the RA.
Carotid Stenting
Access site bleeding and vascular access complications are the most common adverse events after carotid artery stenting (CAS) with TFA. The need for transfusion may significantly increase the stroke risk as well.61 Complex aortic arch is a risk factor for technical failures, and type III aortic arch with friable atheromas is the most risky feature for CAS complications.62 The highest prevalence of atherosclerosis distribution is in the descending aorta (38.2%), followed by arch (27.6%) distal to the innominate artery, especially with increasing age.63 On the other hand, symptomatic stroke (14%) contralateral to the treated carotid stenosis indicates that aortic arch catheter manipulation is a cause of atheroembolic brain lesion.61,64 TRA may minimise catheter contact in the arch, particularly for right ICA and left bovine ICA. Transradial CAS can be successfully performed by experienced operators with a low complication rate in a large percentage of patients.65,66
From a technical point of view, in terms of the type of carotid stent and the required ID of the delivery system, a 6 Fr or 7 Fr guiding catheter may be used. When stents require a larger delivery system or better support is needed, a long 5 Fr or 6 Fr sheath may also be used. Either way, a distal protection filter system can also be used. If a proximal balloon occlusion technique is desired, it also can be done as described above.
Conclusion
TRA has become the standard approach for cardiac intervention due to the large body of evidence demonstrating the lower incidence of vascular complications, better patient experience and cost reduction. The neurovascular field can benefit from the available knowledge from the cardiology field. TRA provides additional tools for the neurointerventionalist and, with adequate training, the whole spectrum of intervention procedures can be carried out. The use of ultrasound is recommended to measure and puncture the RA, as well as to begin the learning curve through performing diagnostic angiography.